Arthritis and Cartilage Injury Treatments
An overview of everything cartilage :
There are three kinds of cartilage all built by the body for different tasks, there is hyaline cartilage most often found in joints, elastic cartilage found in the ear, and fibrocartilage in the spine and the knee meniscus. How all these differ in how much of a substance called collagen they are made of and how that collagen is aligned.
We will focus on articular cartilage ( joint cartilage ) which is very specialized. The collagen that makes up its architecture is built into a sort of netting that is made to hold in water which makes it low friction that allows our joiunts to move freely and smoothly. The bigest problem is that there is very very poor blood flow as you can suspect inside a joint leading to very difficult healing when this joint cartilage is injured. The cells that normally help build the cartilage called chondrocytes do not funtion well in rapaing adult joint catilage. So that a small injury to the smooth cartilage can over time expand and destroy the joint - we call that degenerative arthritis.
Patients present to us with varying degrees of cartilage injury, some exhibit no pain symptoms. others with severe joint pain, some just complain of the joint locking up, weakness and instability in the joint, or joint effusion ( that means joint is swollen ).
First off we take a complete history to make sure there are no systemic diseases that are causing the arthritis ( rhumatoid arthritis, psoriatic arthritis, seronegative arthritis, etc. )
Then we xray to see the overall position of the limb joints to see if there is any deformity that can be causing undue stress on the joints that over time can also destroy the joint cartilage. The xray will also show us the arthritis progression and amount of bone damage. If we find a significant deformity or malalignment on the limbs we sometimes consider realigning the legs to remove the 'deforming' forces. What I mean by that is cartilage and the human joint is built for weight to be placed directly on to it, if there is side to side or a shearing force on the joint the cartilage gets damaged.
Surgical Cartilage Arthritis Repairs:
Not everyone needs surgery, sometimes we can give an injection of cortisone into the joint torelieve inflammation, other times we can prescribe an anti inflammatory medication of make a custom brace.
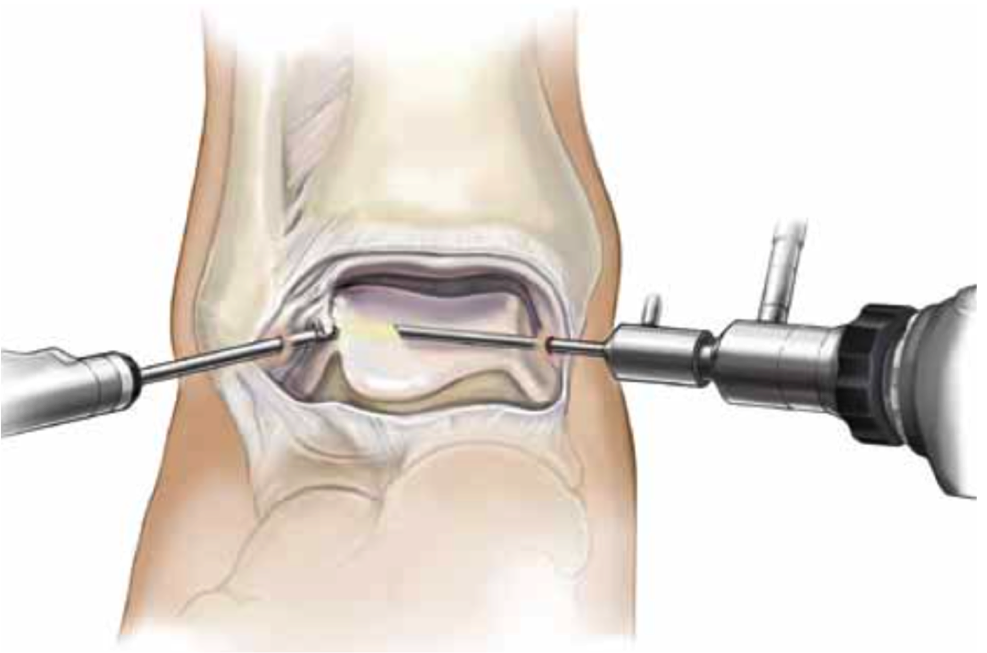
Many times surgery is a great option, if there is a loose piece of cartilage in the joint surgical cleaning of the joints works very well, usually done with arthroscopy ( video camera into to joint through a very small 5 mm incision )
We perform a procedure called microfracture, what we do in this case is fing the cartilage injury with the arthroscope, then drill it to stimulate bleeding after we clean out any loose particles. when it bleeds in the area it forms fibrocartilage. Now fibrocartilage is not as good as the original hyaline cartilage the body put there originally but it does create a painless and smooth surface for that injured joint.
If there is a situation where the cartilage is intact but there is a bone injury under it we can perform a trans-talar drilling. This is an advanced technique where we drill through one of the bones in the foot called the talus while we watch the ankle joint with a scope. We literally drill into the bone injury underneath the cartilage and the nfill the injury with healthy new bone.
Below is a drawing of the procedure im describing, the blue colored device is a special guide we use to position the drill to hit the ankle injury ( also called a talar dome injury )

In more severe cases of injuries to the cartilage on the ankle joint we perform something called an OATS procedure where we take cartilage from the knee joint or even a cadaver cartilage plug and place it into a predrilled patient ankle to replace the injury with new cartilage. It works well in the right cases! you can see pic below of the talus bone with circular grafts in place.

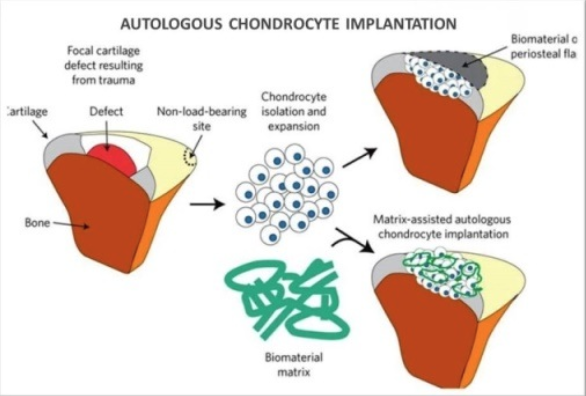
Another new technique we use to fix these cartilage injuries is autologous chondrocyte implantation. Here we harvest hyaline cartilage cells from healthy joint and then reimplant them in the patients damaged ankle injury. Sewn into place with very fine stiches. The advantage of this technique is that hyaline cartilage is produced. That is normal ankle cartilage so we get it as close to normal as possible. This procedure is reserved for very particular cases of large cartilage injury.
In very severe cases we can replace part of a damaged ankle with a fresh cadaver graft. The was this works is we take a CT scan and xrays of a patients ankle, then a special lab finds a donor match of an ankle with the same dimensions. we then cut a peice of the cadaver bone and cartilage and use it to replace a damaged ankle joint . The xrays below shoe on the left a severely arthritic ankle joint .the next two xrays show screws holding in a cadaver ankle. We replaced the entire ankle with a cadaver ankle joint. again patient selection is of utmost importance for this advanced procedure.

We are also working on 2nd generation cell scaffold techniques for cartilage regeneration, the use of growth factors, growth hormone injections to ankle joint, stem cell cartilage replacement and ankle distraction.
What is ankle distraction????
This was popular about 3-4 years ago. An external fixator was applied to the ankle to stretch out the ankle joint and relieve pressure on the joint to stimulate healing. By itself the procedure does NOT have long lasting results that we have found. But - when used with the procedures explained above it may have some promising results. Look at photo below. on the left is a severely arthritic ankle with no joint space on the xray- this is a very bad sign. On the right is an xray of the same ankle during distraction, the joint is literally pulled apart for 6 to 8 weeks and this helps it to heal. Again this is a procedure for very select cases.

And finally in the most severe cases, ankle fusion where we use screws, plates, pins, external fixators and rods to remove the painful arthritic joint completely and render the joint immobile completely. This may sound scary but in advanced cases it is the best route for most patients.
One last thing is ankle replacement- does not work as well as hip and knee replacements. The science and technology is simply not there yet, we do not recommend there procedures at this time ( usually).
We do however do many cases of failed ankle implants. These require extensive surgery, sometimes bone grafting, bone regeneration, bone replacement and external fixation in many cases. The failed ankle implant and the failed fusion with nonunion has become a common repair at this point - unfortunately.
I realize we have presented information on ankles but these techniques work in more foot joints just as effectively.
FLORIDA, NAPLES, FORT MYERS, BONITA SPRINGS, TAMPA, SARASOTA, MIAMI, FORT LAUDERDALE, BOCA RATON, WEST PALM BEACH, NEAR ME, CANADA